(1) Thoracic surgery
Left lung decortication
Day: Tuesday Date: 24/7/2023 Patient gender: male age: 3 years old
the patient had pneumonia in his left lung which developed into empyema
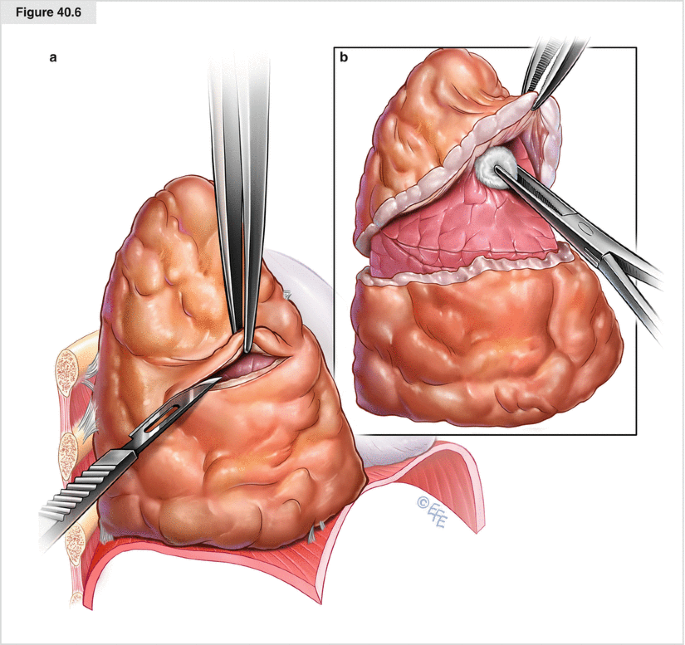
Lung decortication is a simple yet formidable procedure. It involves the excision of the thick fibrinous peel from the pleural surface, thereby permitting the expansion of the underlying lung parenchyma. Patients with long-standing empyema, pleural thickening, hemothorax, and pleural tumors are candidates for decortication.
Technique
- Skin incision: The skin incision swings downwards, beginning at a level midway between the spinous process to the tip of the scapula. The anterior limit is the mid-axillary or anterior axillary line. This incision extends around 2 inches below the tip of the scapula. The incision is deepened using the electrocautery. The latissimus dorsi and the serratus anterior muscles are divided using the electrocautery. The tip of the scapula is grasped using an Allis forceps, and the ribs are counted in the subscapular space.
- Entry into the thoracic cavity is established via the fifth or the sixth interspace. It must be kept in mind that the electrocautery must divide the intercostal muscles at the upper border of the lower rib so that the neurovascular bundle is spared. A rib resection might be required if there is excessive crowding of the ribs.
- After the division of the intercostal muscles, the extrapleural space is entered. Care is taken not to enter the empyema cavity directly. The mediastinum is generally not involved in the inflammatory process. Therefore care must be taken to avoid injury to the mediastinal structures. Similarly, the apex of the lung must be freed carefully.
- Injury to the subclavian vessels may occur during the apical dissection and can cause hemorrhage. Care must also be taken to avoid injury to the esophagus (left-side decortication) or vena cava (right-side decortication) during medial dissection and diaphragm during the inferior dissection. The rind or the pleural peel must be removed from the lung parenchyma, including the fissures
- After removal of the thick peel, the anesthesiologist is asked to inflate the lung to locate the air-leaks. All the major air-leaks must be formally closed with suture. Adequate hemostasis must be ensured. Diathermy or bipolar forceps may be quite handy to achieve hemostasis.
- The intercostal drain is inserted in the thoracic interspace. Some surgeons insert two drains-one in the base (posterior) and one in the apex (anterior). These tubes remain in place until the appearance of signs (clinical and radiological) of lung expansion.
- Subsequently, a layered chest wall closure is done
- beforeafter
.


Comments
Post a Comment